

Nandrolone Decanoate / Testosterone Cypionate / Testosterone Enanthate Injection
Product Overview
Nandrolone Decanoate / Testosterone Cypionate / Testosterone Enanthate Injection is a sterile, oil-based intramuscular formulation that delivers three long-acting anabolic-androgenic steroids in a single 5 mL multidose vial. Each milliliter provides 60 mg of nandrolone decanoate, 70 mg of testosterone cypionate, and 70 mg of testosterone enanthate suspended in grapeseed oil.
Nandrolone is a 19-nor-testosterone analog with a comparatively high anabolic-to-androgenic activity ratio, whereas testosterone cypionate and testosterone enanthate are esterified forms of endogenous testosterone designed for prolonged release after deep-muscle deposition.
Clinically, the combination is prescribed in select cases of symptomatic androgen deficiency that also require anabolic support-such as chronic catabolic states or anemia-when a prescriber judges that a tailored ratio of testosterone to nandrolone may optimize outcomes.[1]
Because there is no FDA-approved, fixed-dose commercial preparation containing all three active ingredients, this medicine is compounded on demand for individual patients under section 503A. The customized approach enables physicians to provide nandrolone therapy-which is no longer marketed in the United States-to patients who still need its anabolic or erythropoietic properties while simultaneously restoring physiologic testosterone levels.
By statute, all three components are Schedule III controlled substances, so dispensing and possession require a valid prescription and careful record-keeping. Available by prescription from a 503A compounding pharmacy.[2]
Therapeutic goals typically include stabilizing or raising serum testosterone into the mid-normal range, improving nitrogen balance, increasing or preserving lean body mass, and boosting red-blood-cell production.
Because androgen therapy carries recognized risks-ranging from prostate stimulation and polycythemia to alterations in lipids and liver enzymes-prescribing clinicians must document a clear clinical indication, obtain baseline laboratory studies, counsel patients on controlled-substance regulations, and provide structured follow-up.[3]
Because the preparation is compounded, dosing is fully individualized. A common starting regimen for hypogonadal men involves 1 mL (total 200 mg steroid content) injected deeply into the gluteal muscle every seven to ten days, approximating mid-physiologic testosterone exposure while providing a modest 60 mg/week nandrolone anabolic adjunct.
Serum testosterone is drawn midway between injections guides titration: clinicians typically target the center of the reference range to avoid supra-physiological peaks.[1]
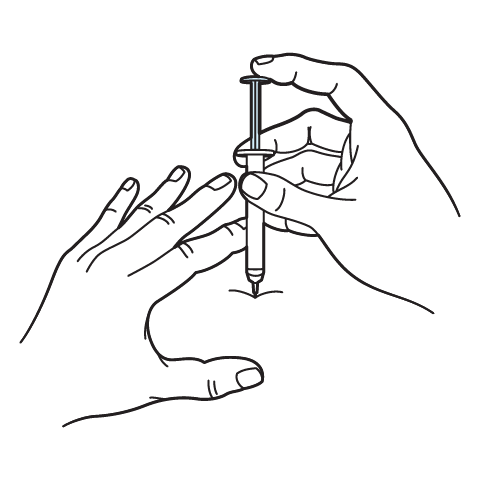
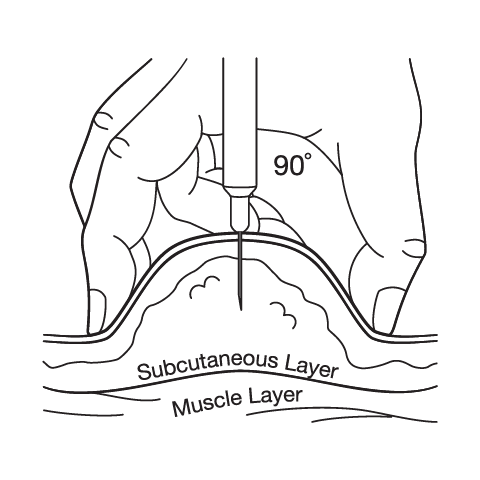
Administration requires a 22- or 23-gauge, 1- to 1.5-inch needle inserted at 90 degrees into well-relaxed muscle. Aspiration prior to injection confirms the absence of blood return. The vial is gently warmed in the hands to reduce viscosity, swabbed with alcohol, and accessed with a new sterile needle for each draw to maintain sterility. Self-administration is feasible after formal instruction, but many patients prefer clinic visits until technique is mastered.[3]
Laboratory surveillance includes hematocrit and hemoglobin at baseline, three months, and then semi-annually; fasting lipid panel annually; liver-function tests yearly; and prostate-specific antigen plus digital rectal examination according to age-appropriate cancer-screening guidelines. Dose reductions or interval extensions are mandated if hematocrit exceeds 54 percent, PSA rises significantly, or LDL cholesterol climbs despite lifestyle measures.[7]
Treatment duration depends on indication. In chronic primary hypogonadism, lifelong replacement may be necessary, whereas patients using the combination for reversible catabolic conditions often taper after clinical goals (weight restoration or hematologic correction) are met.
Physicians occasionally implement drug holidays-eight to twelve weeks off therapy-to permit hypothalamic-pituitary axis recovery and to re-assess the continued need for anabolic support.[2]
Once injected intramuscularly, the grapeseed-oil depot slowly releases each ester into the circulation. Testosterone cypionate and testosterone enanthate are hydrolyzed by esterases to free testosterone, which binds androgen receptors in target tissues such as skeletal muscle, bone, and bone marrow.
Activation of the receptor up-regulates transcription of proteins involved in muscle protein synthesis, mineral retention, and erythropoietin stimulation, thereby explaining increases in muscle mass, bone density, and hematocrit observed during replacement therapy.[4]
Nandrolone decanoate undergoes similar enzymatic cleavage to yield nandrolone, an androgen that binds the same receptor with slightly higher affinity but is less readily converted by 5-α-reductase to the potent androgen dihydrotestosterone. Consequently, nandrolone exerts strong anabolic effects with comparatively muted androgenic stimulation of skin and prostate tissue.
Animal and human studies demonstrate that nandrolone promotes myofibrillar protein synthesis, increases type I collagen deposition in bone, and enhances erythropoiesis, partly via increased renal production of erythropoietin.[5]
When the three esters are co-administered, their pharmacokinetic half-lives overlap (roughly seven to ten days for each), allowing clinicians to maintain relatively stable serum testosterone and nandrolone concentrations using once-weekly or bi-weekly dosing.
Testosterone aromatization to estradiol contributes to bone health but can lead to gynecomastia in susceptible males, while nandrolone’s weaker aromatization profile partially mitigates this estrogenic burden.
Overall, the formulation provides a synergistic anabolic-androgenic milieu that supports tissue repair and endocrine normalization in androgen-deficient states while theoretically lowering the risk of excessive androgenicity compared with higher-dose single-agent testosterone.[6]
Therapy is contraindicated in any patient with known or suspected carcinoma of the prostate or male breast because exogenous androgens can accelerate the growth of hormone-responsive tumors.
It is likewise contraindicated in pregnant women owing to the risk of virilization of a female fetus and other congenital malformations.
Severe hepatic impairment, nephrotic nephrosis, uncontrolled heart failure, and significant coronary artery disease are additional settings where androgen-induced fluid retention or cholestasis could precipitate clinical decompensation.[7]
Individuals with hypersensitivity to any component of the formulation-including grapeseed oil-or with a history of anaphylactoid reactions to injectable steroids must avoid use.
Pediatric patients with open epiphyses are generally excluded because anabolic steroids hasten epiphyseal closure and may stunt final height.
Clinicians must also weigh risks carefully in men with polycythemia or untreated obstructive sleep apnea, as androgen therapy can worsen both conditions by raising hematocrit and altering ventilatory drive.[8]
Because all three ingredients are Schedule III substances, the formulation is unsuitable for anyone with current anabolic-steroid misuse or a history of substance-use disorder without strict oversight.
Baseline evaluation should include digital rectal examination and prostate-specific antigen in men over fifty, liver-function tests, lipid panel, hematocrit, and screening for cardiovascular disease before initiation.
Any emergence of a contraindication during therapy-such as rapidly rising PSA-necessitates immediate discontinuation and further evaluation.[6]
Exogenous androgens heighten the anticoagulant effect of vitamin K antagonists by down-regulating clotting-factor synthesis; patients stabilized on warfarin may therefore require empiric dose reduction and more frequent INR monitoring when injections begin.
Testosterone and nandrolone also increase insulin sensitivity, so diabetic patients receiving insulin or sulfonylureas should monitor glucose closely and adjust antidiabetic therapy to avoid hypoglycemia.[7]
Co-administration with systemic corticosteroids or ACTH creates additive sodium and water retention, risking oedema and hypertension in susceptible individuals.
Androgens can alter thyroid-binding globulin concentrations, yielding lower total T₄ yet unchanged free hormone; clinicians interpreting thyroid tests must recognize this laboratory artefact.
High-dose or illicit stacking of additional anabolic steroids or growth hormone is discouraged, because unpredictable endocrine synergy dramatically raises risks of hepatotoxicity, dyslipidemia, and cardiomyopathy.[8]
Laboratory assays can be confounded: serum creatinine and creatine-kinase values often rise as muscle mass increases, and hematocrit typically climbs within three months. These changes are physiological within limits but may mask renal injury or myopathy if baseline values are unknown.
Regular, structured monitoring of coagulation, glucose, electrolytes, hematocrit, and lipids is essential to manage interactions safely.[8]
Androgen therapy can provoke a wide continuum of adverse effects. Endocrine sequelae dominate negative feedback at the hypothalamic-pituitary-gonadal axis suppresses luteinizing and follicle-stimulating hormone, leading to oligospermia, testicular atrophy, and potential infertility in men.
Estradiol generated via aromatization may induce tender gynecomastia, whereas women exposed inadvertently risk virilizing changes such as deepened voice, hirsutism, and menstrual irregularity. Many manifestations regress after withdrawal, but voice and clitoral enlargement can be permanent.[5]
Dermatologic complaints include seborrheic acne and accelerated male-pattern alopecia. Androgen-stimulated sebaceous glands produce more sebum, predisposing to inflammatory lesions-particularly on the back and shoulders. Hair follicles sensitive to dihydrotestosterone miniaturize, producing patterned baldness that often persists despite discontinuation.
Mood alterations range from euphoria or irritability to anxiety, insomnia, or depressive symptoms, likely related to steroid modulation of central neurotransmitter systems.[8]
Cardiometabolic liabilities are well documented: injectable androgens lower high-density lipoprotein and raise low-density lipoprotein cholesterol, fostering a pro-atherogenic lipid profile. They increase red cell mass, occasionally causing polycythemia, which escalates thrombotic risk. Fluid and sodium retention may elevate blood pressure and precipitate heart-failure exacerbations. Rare cases of myocardial infarction and cerebrovascular accident have been reported in long-term or high-dose users, especially when combined with other cardiovascular risk factors.[5]
Although 17-alkylated oral steroids are more notorious for hepatotoxicity, parenteral nandrolone and testosterone have nonetheless been linked-rarely-to cholestatic jaundice, peliosis hepatis, and hepatic adenoma. Vigilant monitoring of aminotransferases and bilirubin is prudent during extended courses.
Local reactions are usually mild-transient soreness or redness at the injection site-but sterile abscesses or cellulitis can develop if asepsis is breached. Prompt medical attention is warranted for any persistent pain, swelling, or systemic signs of infection.[9]
This medication is strictly contraindicated in pregnancy. Animal data and human case reports show that first-trimester androgen exposure can masculinize external genitalia of a female fetus and impair normal gonadal development.
Category X designation reflects evidence of fetal risk that outweighs any conceivable maternal benefit. Women of child-bearing potential must demonstrate a negative pregnancy test before starting treatment and employ reliable contraception throughout therapy.[4]
Lactation safety is undetermined, but androgens are likely excreted in breast milk and could disrupt neonatal endocrine balance; therefore, breastfeeding while on therapy is discouraged.
Both men and women should also recognize that supraphysiologic androgen exposure may transiently impair fertility-by suppressing spermatogenesis in men and by inhibiting ovulation in women-requiring months for full recovery after discontinuation.[4]
Store the vial upright at controlled room temperature, 20 - 25 °C (68 - 77 °F), protected from light. Do not refrigerate or freeze: cold temperatures thicken grapeseed oil and may cause drug precipitation, while freezing can fracture the container.
After each use, wipe the stopper with alcohol and return the vial to its carton or an opaque container to minimize light exposure.[10]
Discard any solution that appears cloudy, contains particulates, or changes color. Observe the beyond-use date assigned by the compounding pharmacy and dispose of expired medication through authorized drug-take-back programs or in accordance with local regulations-never via household trash or plumbing.
Used needles belong in a puncture-resistant sharps container. Keep the vial and all administration supplies in a locked area inaccessible to children, pets, and unauthorized individuals.[10]
- DailyMed. (2024). Testosterone cypionate injection USP [Prescribing information]. National Library of Medicine. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=2d067e21-c5c7-4baf-acb8-51b9e7354f4a
- National Center for Biotechnology Information. (2023). Nandrolone decanoate (CID = 92771) in PubChem. https://pubchem.ncbi.nlm.nih.gov/compound/92771
- Pan, M. M., & Kovac, J. R. (2016). Beyond testosterone cypionate: evidence behind the use of nandrolone in male health and wellness. Translational Andrology and Urology, 5(2), 213-219. https://doi.org/10.21037/tau.2016.03.03
- Bhasin, S., Brito, J. P., Cunningham, G. R., et al. (2018). Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. Journal of Clinical Endocrinology & Metabolism, 103(5), 1715-1744. https://doi.org/10.1210/jc.2018-00229
- Patanè, F. G., Liberto, A. N. M., Maglitto, A. N. M., et al. (2020). Nandrolone decanoate: use, abuse and side effects. Medicina, 56(11), 606. https://doi.org/10.3390/medicina56110606
- U.S. Drug Enforcement Administration. (2024). Controlled substances schedules. https://www.deadiversion.usdoj.gov/schedules/
- Mayo Clinic. (2025). Testosterone cypionate (intramuscular route). https://www.mayoclinic.org/drugs-supplements/testosterone-cypionate-intramuscular-route/description/drg-20563731
- Basaria, S. (2010). Androgen abuse in athletes: detection and consequences. The Journal of Clinical Endocrinology & Metabolism, 95(4), 1533-1543. https://doi.org/10.1210/jc.2009-1579
- Swerdloff, R. S., & Wang, C. (2012). Anabolic steroid abuse: pathophysiology and effects on the hypothalamic-pituitary-testicular axis. Endocrinology and Metabolism Clinics of North America, 41(4), 749-762. https://doi.org/10.1016/j.ecl.2012.08.002
- United States Pharmacopeial Convention. (2023). USP <797> Pharmaceutical compounding-sterile preparations. https://www.usp.org/compounding
- American Urological Association. (2022). Testosterone Deficiency Guideline. https://www.auanet.org/guidelines-and-quality/guidelines/testosterone-deficiency-guideline
- Bagchus, W. M., et al. (1987). Hormone kinetics after intramuscular testosterone cypionate administration. Journal of Clinical Endocrinology & Metabolism, 65(1), 1-7. https://pubmed.ncbi.nlm.nih.gov/3595893/
- StatPearls. (2024). Intramuscular injection. National Center for Biotechnology Information. https://www.ncbi.nlm.nih.gov/books/NBK556121/
- Centers for Disease Control and Prevention. (2024). Vaccine Administration-Pink Book: Chapter 6. https://www.cdc.gov/pinkbook/hcp/table-of-contents/chapter-6-vaccine-administration.html
- Defy Medical. (2025). Testosterone Cypionate 200 mg/mL (Grapeseed Oil) - Storage Information. https://www.defymedicalstore.com/32
- World Anti-Doping Agency. (2024). GC/C/IRMS analysis of testosterone and nandrolone metabolites after a 150 mg nandrolone decanoate dose. https://www.wada-ama.org/en/resources/scientific-research/gccirms-analysis-testosterone-and-nandrolone-metabolites-after
- Shoskes, D., et al. (2021). Utilization and impact of aromatase-inhibitor therapy in men on testosterone replacement. Sexual Medicine, 9(3), 100461. https://pmc.ncbi.nlm.nih.gov/articles/PMC8360915/
- StatPearls. (2024). Biochemistry, dihydrotestosterone. National Center for Biotechnology Information. https://www.ncbi.nlm.nih.gov/books/NBK557634/
- Hartgens, F., & Kuipers, H. (2004). Body composition changes with nandrolone decanoate in resistance-trained men. European Journal of Applied Physiology, 81(1-2), 1-8. https://pubmed.ncbi.nlm.nih.gov/15076791/
- Solanki, P., et al. (2023). Recovery from anabolic steroid-induced hypogonadism: a scoping review. Endocrine Connections, 12(12), e230358. https://pubmed.ncbi.nlm.nih.gov/37855241/
How often do I have to inject this medication?
Most patients maintain stable hormone levels with a deep-muscle injection of 1 mL every 7 - 10 days; your prescriber will individualize the schedule based on mid-cycle labs.[11]
When do testosterone levels peak and fall after each shot?
Serum testosterone typically rises above baseline within 2 - 3 days and drifts back toward pre-injection values by days 13 - 14.[12]
What needle size and site are best for this thick oil?
Current technique guidelines recommend a 22- or 23-gauge, 1- to 1.5-inch needle inserted at 90 ° into a large muscle (ventrogluteal or dorsogluteal) for volumes up to 1 mL.[13]
Do I need to rotate injection sites?
Yes-alternating between left and right ventrogluteal or vastus lateralis areas reduces scarring and lowers the risk of sciatic-nerve injury.[14]
How should I store the vial if my home gets cold?
Keep it at normal room temperature (68 - 77 °F); refrigeration or freezing can cause the testosterone to crystallize and make injection painful.[15]
Will this medication make me fail an athletic drug test?
Nandrolone metabolites can remain detectable in urine for up to nine months after a single dose, so the formulation would trigger a positive steroid screen during that window.[16]
Do I need an aromatase inhibitor while on therapy?
Only men whose estradiol exceeds ~60 pg/mL or who develop estrogen-related symptoms benefit from low-dose anastrozole; routine prophylaxis is unnecessary.[17]
Can this injection speed up hair loss?
Any treatment that raises testosterone can also raise dihydrotestosterone-the androgen linked to male-pattern baldness-so genetically susceptible users may notice accelerated thinning.[18]
How soon will I see gains in muscle or strength?
Controlled studies show measurable increases in lean mass within 6 - 8 weeks of nandrolone supplementation when combined with resistance training.[19]
If I stop, how long until my fertility returns?
Most men regain near-baseline gonadotropin levels within 3 - 6 months, but full spermatogenesis can take several months to a year, depending on duration and dose.[20]
Administration Instructions
Intramuscular Injection Instructions
Subcutaneous Injection Instructions
 Nandrolone Decanoate Injection
Nandrolone Decanoate Injection Oxandrolone Tablets
Oxandrolone Tablets Oxandrolone Troches
Oxandrolone Troches Testosterone Cypionate Injection
Testosterone Cypionate Injection Anastrozole Capsules
Anastrozole Capsules Enclomiphene Citrate Capsules
Enclomiphene Citrate Capsules HCG Injection
HCG Injection Sermorelin Acetate Injection
Sermorelin Acetate Injection503A vs 503B
- 503A pharmacies compound products for specific patients whose prescriptions are sent by their healthcare provider.
- 503B outsourcing facilities compound products on a larger scale (bulk amounts) for healthcare providers to have on hand and administer to patients in their offices.
Frequently asked questions
Our team of experts has the answers you're looking for.
A clinical pharmacist cannot recommend a specific doctor. Because we are licensed in all 50 states*, we can accept prescriptions from many licensed prescribers if the prescription is written within their scope of practice and with a valid patient-practitioner relationship.
*Licensing is subject to change.
Each injectable IV product will have the osmolarity listed on the label located on the vial.

Given the vastness and uniqueness of individualized compounded formulations, it is impossible to list every potential compound we offer. To inquire if we currently carry or can compound your prescription, please fill out the form located on our Contact page or call us at (877) 562-8577.
We source all our medications and active pharmaceutical ingredients from FDA-registered suppliers and manufacturers.